
Diabesity is so-named because of the close association of obesity and diabetes (type 2). Obesity typically comes first and type 2 diabetes comes later. This leads many to conclude that obesity causes diabetes. On the surface, this seems reasonable, since the two often co-exist. Where it becomes more difficult, however, is when people try to explain why and how obesity causes diabetes.
Here, the answers become much more vague. Some hypothesize that fat cell produce hormones that somehow, magically cause diabetes. Some suggest that fat cells produce a hormone called pigment epitelium-derived factor that causes insulin resistance. But why would fat cells start producing this hormone in the first place?
Some researcher think that fat cells produce a hormone called resistin that causes other cells to become insulin resistant. Clever name, guys. But why would fat cells produce this hormone in the first place?
Others, such as researchers from Harvard, think that obesity ‘stresses out’ the cells like an unruly pimple in high school. This – for some reason- makes the cells send out a signal that insulin receptors should stop responding to insulin. This causes insulin resistance. Really? That’s the best you can come up with?
The answer, though, is much simpler and its roots lie in the Hormonal Obesity Theory.
We’ve previously explored the evidence supporting the Hormonal Obesity Theory so far. Insulin is the main driver for obesity. Cortisol plays a role as well, but insulin is the major player for most people. Insulin also increases insulin resistance in a self reinforcing cycle.
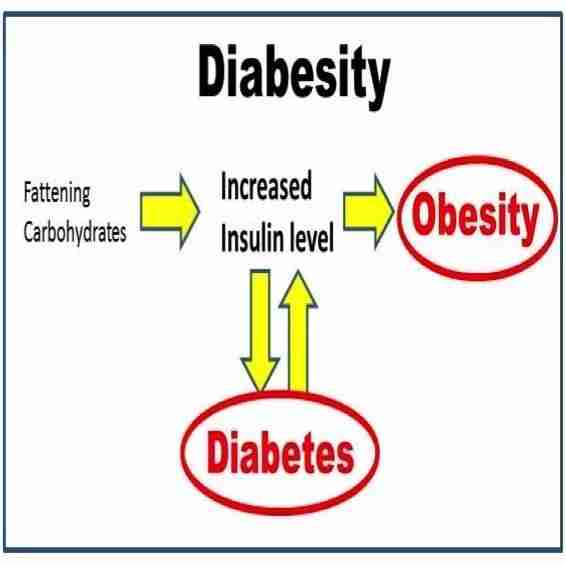
Since type 2 diabetes is really another word for insulin resistance, we can rearrange the Hormonal Obesity Theory this way.
Under this construct, both obesity and diabetes are caused by the same thing – high insulin levels. That explains why diabetes and obesity are so tightly associated. It also explains why all efforts to find how obesity causes diabetes have failed. That is because obesity doesn’t cause type 2 diabetes. They are instead both manifestations of hyper-insulinemia. It turns out that the entire metabolic syndrome relates to high insulin levels, but we will explore that in the future.
Diabetes and obesity both have a common cause – high insulin levels. They are essentially two sides of the same disease hence the name – diabesity. We can also see that there is an interesting chicken and egg problem here. Insulin leads to insulin resistance which leads to insulin in a vicious circle. So what comes first?
Is the problem started by insulin resistance due to, say, genetics? Or is the problem high insulin to start? Both are possible. Obesity typically manifests first. So we can start to solve the problem by looking at the time course of obesity, particularly juvenile obesity.
In this paper “Early Changes in Postprandial Insulin Secretion, not in Insulin Sensitivity Characterize Juvenile Obesity“Diabetes 43:696-702; 1994 Le Stunff C, the authors looked at 3 groups of people – non-obese, recent obesity (<4.5 years) and long standing obesity (>4.5 years). They were able to measure insulin secretion in response to a standardized meal.
As you can see, both groups of obese subjects had higher levels of insulin secretion compared to the non-obese. Abnormally high insulin secretion develops early in the course of obesity and persists.
What about insulin resistance?
Looking at the accompanying charts, you can see that insulin resistance (measured here by maximal glucose uptake) develops over time. With longer duration of obesity, insulin resistance increases. The insulin resistance now contributes more and more to the fasting insulin levels.
This is the answer to the chicken and egg question of insulin and insulin resistance. Insulin is the primary insult. Persistent high levels of insulin leads to insulin resistance. This insulin resistance in turn leads to higher insulin levels.
The time sequence of juvenile obesity can be represented like this. What this really looks like is our understanding of Hormonal Obesity Theory.
Last week there was some excitement with the report published in the Journal of the American Medical Association that obesity rates for the age group 2-5 years had dropped by 43%. Most other age groups did not see a significant change in rates of obesity. Since childhood obesity is highly linked to adult obesity, this is indeed very good news.
Some groups, such as Michelle Obama’s misguided Let’s Move campaign wasted no time in congratulating themselves on a job well done. They believe that their campaign of physical activity has played a key role in this success. This is despite the fact that most studies show that exercise has little or nothing to do with weight loss.
If their anti-obesity programs were such a success, why do we only see results in the lowest age group (age 2-5)? I don’t ever recall thinking that most 2 year olds need to be more active. I don’t recall seeing any 2 year olds in the gyms pumping iron, either. Adult obesity, though, don’t seem to have been much changed. The answer, though is much more straightforward. It lies in the time dependent effects of obesity.
Those with long standing obesity tend to have more insulin resistance and therefore harder-to-treat obesity. The relatively short duration of obesity of the 2-5 year old group means that obesity is relatively easier to treat.
If we look at the Total caloric sweeteners line, we see that from 1977 to 2000 there has been a steady increase in per capita sweetener consumption. This was in response to the odious Dietary Guidelines of 1977 which produced the infamous food pyramid. The goal was to eat lower and lower fat as a percentage of calories and more carbohydrates. So sugary foods, as long as they were low in fat, were encouraged. 1977 is also when the obesity epidemic started.
Sweetener consumption peaked in 2000 under the Atkins onslaught. In the late 1990′s and early 2000s the Atkins cuisine reigned supreme. This included all the wannabe Atkins imitators. All of the attention paid to the low-carb message resulted in lower sweetener intake due to the realization that sugar makes you fat.
Of course, you could have simply asked your grandmother. She would have told you that the first step in losing weight was to stop eating sweets and starchy foods. Instead, we listened to the politicians and the doctors who said that sugar didn’t make you fat, fat made you fat. Even as we ate lower and lower fat, we gained more and more weight.
The key benefit of the Atkins message was that sugar intake started to fall starting in the year 2000. Even after the Atkins craze became as unfashionable as a Livestrong bracelet, the undeniable truth was that too much sugar was bad for you. Really, really bad. Sugar intake falls in year 2000 and after a 5-10 year lag, so does obesity in the most easy-to-treat group. Makes perfect sense to me.
Continue to Hormonal Obesity XII
Begin here with Calories I
See the entire lecture – The Aetiology of Obesity 2/6 – The New Science of Diabesity

By The Fasting Method
For many health reasons, losing weight is important. It can improve your blood sugars, blood pressure and metabolic health, lowering your risk of heart disease, stroke and cancer. But it’s not easy. That’s where we can help.










Responses