
In the early 20th century, cancer didn’t attract much attention. The biggest health problems were infectious diseases — pneumonia, gastrointestinal and tuberculosis. The American Society for the Control of Cancer was created in 1913 and stressed the importance of early detection and aggressive treatment. In the 1940s, they championed the routine use of the Pap smear for cervical cancer. It was hugely and stunningly successful as death rates from cervical cancer dropped quickly. This was an auspicious start. In 1944, the ASCC changed its name to the American Cancer Society.
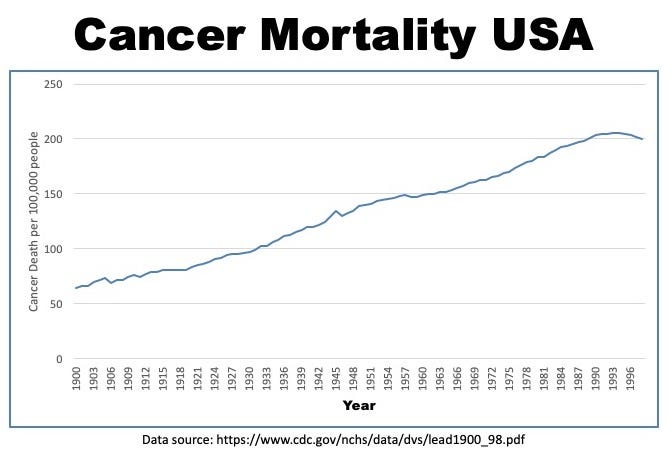
But deaths from infections would drop precipitously over the first half of the century due to improving sanitation and the momentous discovery of antibiotics. Increasing life expectancy meant that heart disease and cancer became increasingly important diseases. Since 1900, the death toll from cancer steamed relentlessly forward like a runaway freight train. The public was starting to notice, and was getting justifiably concerned.
Finally, deciding that enough was enough, then President of the United States, Richard Nixon declared war on cancer in 1971. His State of the Union address actually never mentioned the word ‘war’, instead he proposed “an intensive campaign to find a cure for cancer”. He signed The National Cancer Act into law and injected nearly $1.6 billion into cancer research. Optimism ran high. America had just put a man on the moon with the Apollo program. They had ushered in the atomic age with the Manhattan Project. Cancer? Pffff… that was child’s play. Some scientists enthusiastically predicted that cancer would be cured in time to celebrate America’s Bicentennial in 1976.
The Bicentennial came and went, and the cure for cancer was no closer to being found. By 1981, the 10th anniversary of the war on cancer, the New York Times wondered whether this decade long war “brought real progress against this dreaded disease, or has it been an extravagant $7.5 billion misfire?” Cancer deaths continued their ruthless climb, and the past decade’s efforts hadn’t even slowed its ascent one bit. The ‘war on cancer’ was a complete rout.
This was not news to insiders, like the National Cancer Institute’s (NCI) Dr. John Bailar III. He was also a consultant to the New England Journal of Medicine (then and now, still the most influential medical journal in the world) and a lecturer at Harvard’s School of Public Health. In the 1970s, Dr. Bailar III started to question the effectiveness of the entire cancer research program eventually leaving the NCI in 1980. He pondered this question of what real progress had been made against cancer in an editorial in the New England Journal of Medicine.
In the two decades from 1962 to 1982, the number of Americans who died of cancer increased by 56%. Adjusting for the increased population, this still represented a 25% increase in the rate of death from cancer, at a time when virtually every other disease showed decreasing mortality. Bailar III noted that the data “provide no evidence that some 35 years of intense and growing efforts to improve the treatment of cancer have had much overall effect on the most fundamental measure of clinical outcome — death. Indeed, with respect to cancer as a whole, we have slowly lost ground”. He wondered aloud “Why is cancer the only major cause of death for which age-adjusted mortality rates are still increasing?”
As an insider on the cancer wars, published in the most prominent medical journal in the world, he had yelled out ‘The emperor has no clothes’ in the hopes of energizing new thinking and new research in the stultifying morass of cancer research, which had been mummifying in reiterations of the same cancer paradigms that had failed so utterly. Bailar III just took the first step to fixing a problem, which is admitting that one exists.
But the rest of the cancer establishment was not yet ready to admit a problem. His article received heavy criticism, being called “erroneous’ at best, and ‘reprehensible’ at worst. In the polite world of academia, this language was tantamount to the highest profanity. Dr. Bailar III became almost universally reviled within the cancer research community he had once lead. His motives and intelligence were routinely questioned. Vincent DeVita Jr, then the NCI director, called his first paper reprehensible, irresponsible and misleading while implying that Bailar himself had “departed with reality”. The president of the American Society of Clinical Oncology called Bailar “the great naysayer of our time”. The personal attacks were plentiful, but there was simply no denying the statistics.
In the previous four decades, due to steady improvements in public health, sanitation and medical science, the crude death rate from things other than cancer dropped by 24%. Deaths from cancer increased 14%. The problem of cancer was indeed getting worse but nobody wanted to acknowledge it. The cancer researcher community responded to the message that cancer situation was deteriorating, by killing the messenger. Everything is awesome, they said, even as the bodies piled up.
Little had changed 11 years later, when Dr. Bailar III published a follow up paper called ‘Cancer Undefeated”. The death rate from cancer had increased by another 2.7% from 1982 to 1994. The war on cancer was not just a rout, it was a massacre. Yet still, the cancer world still could not admit there was a problem with their current research. Yes, there were some notable successes. Cancer death rates for children had dropped by about 50 percent since the 1970s. But cancer is the quintessential disease of aging, so this was a major victory in a minor skirmish. Of the 529,904 deaths due to cancer in 1993, only 1699 (3%) were in children. Cancer was delivering punishing upper cuts to our face, and we had managed to tousle Cancer’s fancy hairdo.
The war on cancer was reinvigorated by the continuing revolution in genetics throughout the 1980s and 1990s. Aha! Cancer, we thought, is a genetic disease. Perhaps at long last, we knew our ancient enemy. We opened a new front in the war on cancer, focusing our efforts on finding cancer’s genetic weaknesses. A massive multinational collaboration that saw the 2003 completion of the Human Genome Project would be the first step cure cancer, we thought. This culmination of genetic knowledge that would lay out a battlefield map against cancer. But this historic milestone came and went, and we were no further in our war. An even more ambitious scheme, The Cancer Genome Atlas (TCGA) was hatched. Not only 1 human genome would be mapped, but hundreds. But this, too came and went.
We believed the war on cancer would be a high-tech war of laser beams, smart weapons and nuclear arsenals. Instead, it was reminiscent of the trench warfare of World War I. The front lines never moved, the war dragged on without noticeable progress, and the bodies piled up.
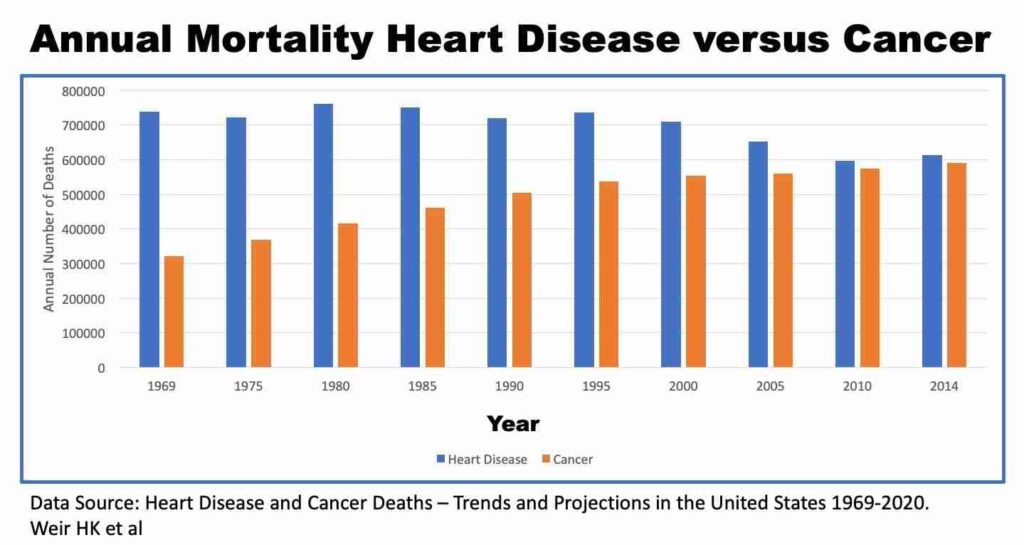
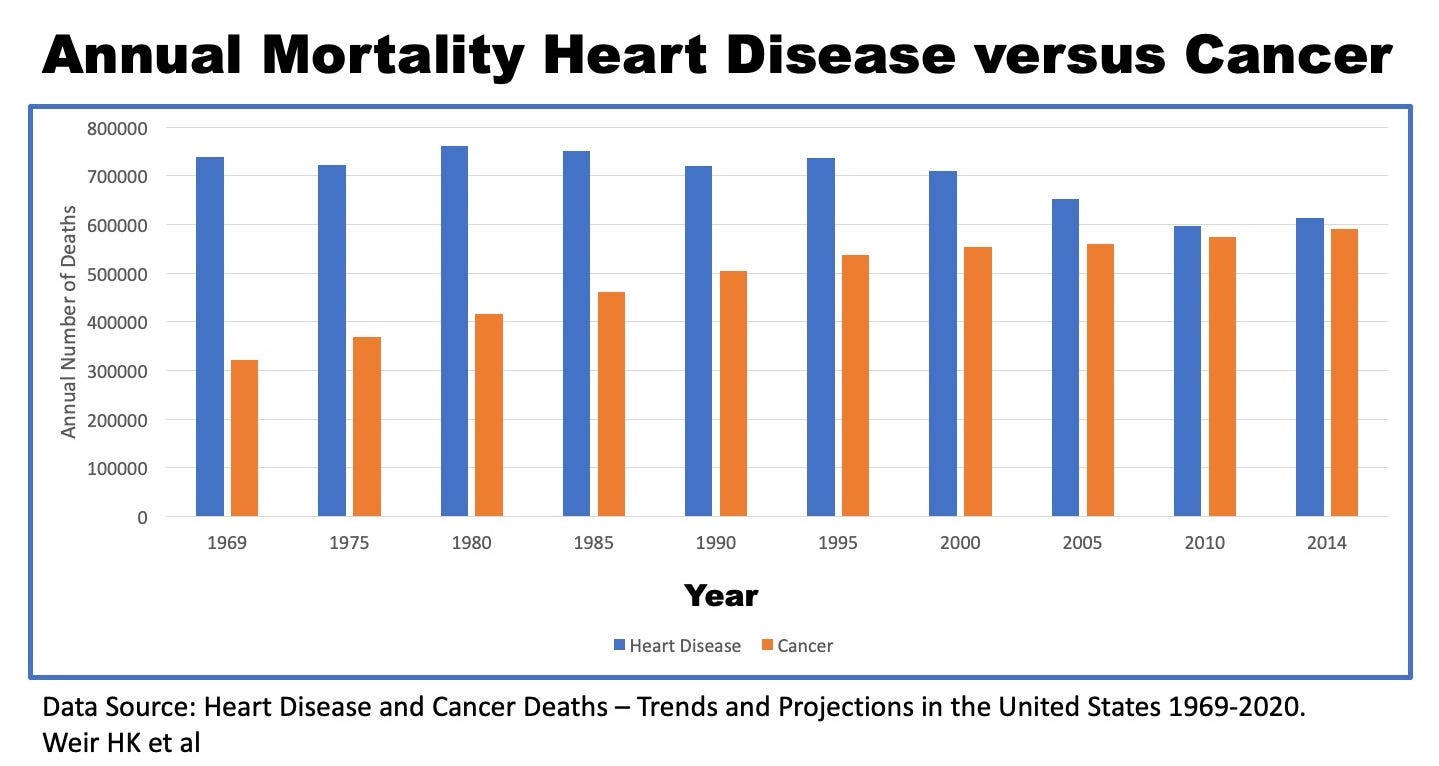
The filibuster in cancer stands in stark contrast to the dizzying progress in other areas of medicine. From 1969–2014, total deaths from heart disease dropped approximately 17% despite the increasing population base in the United States. But cancer? Well, cancer is a problem. During that same time period, deaths from cancer rose a chilling 84%.
By 2009, the New York Times now proclaimed that “Advances Elusive in the Drive to Cure Cancer” noting that the adjusted death rate for cancer had dropped only 5% from 1950 to 2005, compared to heart disease deaths, which had dropped 64% and for flu and pneumonia, which had dropped by 58%. Once again, an American president, this time Barack Obama promised to “launch a new effort to conquer a disease that has touched the life of nearly every American, including me, by seeking a cure for cancer in our time.” Nobel Prize laureate James Watson, the co-discoverer of the double helix of DNA, ruefully noted in 2009 that cancer killed 560,000 Americans in 2006, more than 200,000 more than in 1970, the year before the ‘war’ began.
The costs have been far from insignificant. The 2019 budget for the National Cancer Institute is $5.74 billion, all of which came from tax revenue. Non-profit organizations have proliferated like mushrooms after a rainstorm. By one count, there are more non-profits dedicated to cancer than those for heart disease, AIDS, Alzheimer’s disease and stroke. Combined. In 2013, there were 339 cancer charities in Canada pulling in a massive $644 million. These non-profits are funded by the multitude of Walks for Cancer, to pink ribbon campaigns to Stand Up to Cancer Telethons to the Race for the Cure in New York’s Central Park.
In the United States,the American Cancer Society (ACS) generates over $800 million per year in donations to fund ‘the cause’. While we often think about thousands of volunteers working hand in hand to cure cancer, the reality is far less idyllic. In 2016, the ACS paid 368 employees more than $100,000 each. The former chief operating officer Gregory Bontrager was paid $2,343,992. The lowest paid member of the leadership team took home almost half a million dollars in 2016. The LOWEST paid. Gary Reedy, the CEO paid himself a total package of $820,777. It’s little wonder that pessimists call this ‘Cancer Inc.’ While encouraging all the little old men and women to donate their last $10 for one of their lucrative ‘Relays for Life’, these executives were gorging at the massive bosom of Cancer Inc. But isn’t the ACS a non-profit? Of course. It’s hard to make profits when you are paying executives like they’re Steve Jobs.
But what about all these cancer breakthroughs we keep hearing about? Many new cancer medications didn’t even exist years ago. Surely these shiny new weapons must be helpful in the war on cancer. Well, yes and no. They certainly have made a difference, but not a big one. Cancer drugs are approved in the United States by the Federal Drug Administration (FDA) if they show efficacy with minimal side effects (toxicity). But efficacy can be defined in many different ways.
The gold standard is to prove that new cancer drugs allow patients to live longer. But there are other ways to call a drug effective. Unfortunately, from 1990-2002 (Ref: J Clin Oncol 2003 Apr 1;21(7):1404-11. End points and United States Food and Drug Administration approval of oncology drugs. Johnson JR et al) fully 68% of the FDA approvals for cancer drugs were given for those other reasons. If these drugs did not improve survival, what did they actually do? The most common reason for approval is called the ‘partial tumor response rate’, which means that the primary tumor shrank in volume by over 50%. That sounds pretty good except that this measure is completely irrelevant to a patient’s health.
Cancer is deadly because of its propensity to spread, or metastasize. Cancer kills because it spreads, not because it is big. There is a subset of cancers that don’t metastasize, which are called ‘benign’ because they very rarely cause significant disease. Cancers that metastasize are called ‘malignant’ because of their propensity to kill. Often, benign cancers aren’t even called cancer, but a tumor, which is defined as a collection of abnormal cells, whether benign or malignant.
For example, the very common lipoma, affecting approximately 2% of people at age 50, is a benign cancer of fat cells. It may grow to reach sizes up to 40 pounds. Yet despite this enormous bulk, this benign cancer is still not life-threatening. On the other hand, a malignant melanoma (a type of skin cancer) may weigh only 0.1 pounds and be thousands of times deadlier because of its propensity to spread. Once spread throughout the body, many cancers become unstoppable.
For this reason, local cancer treatments such as surgery or radiation are useless once a cancer has metastasized. Surgeons go to great lengths in the quest to ‘get it all’. They will cut huge swaths of normal tissues out of cancer patients to remove even the faintest rumor of a whiff of cancer cells. Surgery for cancer is only performed to prevent metastasis, not because the cancer is too big. A cancer medication’s ability to reduce the size of a tumor is irrelevant to overall survival. It is analogous to doing surgery to remove half of the cancer – almost completely useless. Every surgeon in the world would refuse to operate because it’s just stupid. And they would be correct. Getting half the cancer is no better than getting none of it.
Yet, the majority of new cancer drugs were approved based solely upon this completely useless marker of ‘efficacy’. From 1990-2002, 71 new drug approvals were granted, although due to approvals for multiple cancers, this only translated into 45 new drugs. Defining efficacy more rigorously as actually saving lives, only 12 medications cleared this bar in the 12 years from 1990-2002. These drugs mostly only extended life by only a few weeks or months. In that same time, the phrase ‘cancer breakthrough’ appeared in 691 published articles. The strange math goes like this:
691 breakthroughs = 71 cancer drug approvals = 45 drugs = 12 drugs that barely extended patients’ lives
All these shiny new weapons in the war on cancer amounted to a jeweled handle on a broken sword. It looked great, but is largely useless. That’s just the way it is for Cancer Inc.

By The Fasting Method
For many health reasons, losing weight is important. It can improve your blood sugars, blood pressure and metabolic health, lowering your risk of heart disease, stroke and cancer. But it’s not easy. That’s where we can help.










Responses